

Ijraset Journal For Research in Applied Science and Engineering Technology
Ergonomics Intervention at Conservation Tourism Trekking Activities to Decrease Tourists\' Risk of Fatigue and Musculoskeletal Disorders (MSDs)
Authors: I Ketut Gde Juli Suarbawa, M. Yusuf, Lilik Sudiajeng
DOI Link: https://doi.org/10.22214/ijraset.2024.63099
Certificate: View Certificate
Abstract
Tourists aim to derive satisfaction and comfort when traveling, although they may experience fatigue. Satisfaction and fatigue are not always correlated, as individuals may feel tired but satisfied and comfortable on a trip. Therefore, the quality of tourism can be improved through the application of ergonomics to reduce fatigue and risk of musculoskeletal disorders. The first phase of this research was conducted on 100 participants who met the inclusion criteria and expressed willingness to serve as the control group. Trekking activities during phase one were carried out according to established procedures without any ergonomics intervention. The second phase was conducted on 100 participants who met the inclusion criteria and showed willingness to be part of the treatment group. The results showed ergonomics intervention in the form of implementing a short break of 3 minutes every 1 hour, providing information in the form of occupational health and safety (OHS) signs relating to danger warnings, evacuation routes, warnings, and prohibitions along trekking route, had an effect on reducing workload during trekking activities. This intervention also significantly reduced fatigue and musculoskeletal disorders.
Introduction
I. INTRODUCTION
There are two trekking routes in Munduk Village conservation tourism area, namely through Subak Dayang and Subak Lampah. Each route covers approximately 4 km and requires about 4 hours to complete, passing three waterfalls, namely Melanting, Labuhan Kebo, and Red Coral. Trekking tourism is related to the perception of destination safety risk, as well as the suitability of the climate, which contributes to the destination's image [1]. Moreover, tourism sector has various risks, including fatigue or physical injury from strenuous and dangerous activities, psychological risk, as well as other negative impacts [2]. Several individuals perceive risks differently, with higher perception influencing travel decisions [3]. Engaging in activities for a duration of 4 hours can lead to musculoskeletal injury, a cumulative disorder characterized by discomfort and pain, resulting in reduced physical capabilities and productivity [4].
Tourists' pursuit of satisfaction and comfort is crucial in tourism. Satisfaction and fatigue are not always correlated, as tourists may feel tired but satisfied and comfortable. Improving tourism quality requires creative methods to minimize "fatigue" while maximizing "satisfaction", which is crucial for the success of the sector, specifically in a competitive landscape [5]. Tourists' fatigue is a common but complex condition characterized by decreased physical function, motivation, emotions, and cognitive abilities [6]. Alzahrani (2019) found a positive relationship between ergonomics and job satisfaction [7], recommending proactive measures through Design Ergonomics [8]. The application of ergonomics provides a fit between people and their work, ensuring tools, information, tasks, and environments are suitable for humans, [7], considering performance abilities and capacities [9]. To address ergonomics issues related to human work activities, the following methods should be used [10], namely (a) Identify current and potential musculoskeletal disorders and related factors through workplace analysis, (b) Define the problem as well as establish what is most prioritized in reducing the identified musculoskeletal disorders, (c) Gather information through observation, video recordings, checklists, direct interviews, and documentation analysis, (d) Assess the problem, (e) Control problems by implementing ergonomics intervention programs such as workstation redesign, changes in work methods, and training, (f) Installation of up-to-date systems.
Previous research on developing tourists’ villages through Kansai Engineering method showed that MEAD concept integrated existing components by formulating and establishing a vision & mission, as well as orders or work directions, and Standard Operating Procedures (SOPs).
This method can help improve the preservation of local wisdom, empower the community, and foster progress in accordance with the village's character [11]. While good product design may suffice for tourism object managers, it is sufficient for tourists, necessitating the integration of health and safety experience with tourism product design [12]. Investigations on waterfalls in Gianyar, Bali, descriptively showed that tourists often experienced accidents such as slipping due to the lack of signs and non-compliance with established standards by the management [13]. Efforts to improve tourism quality by reducing fatigue and risk of musculoskeletal disorders can be carried out through the application of ergonomics. According to Singh, A., & Singh, VK (2022), risk assessment and control positively correlated with Employees retention and efficiency [14]. Ergonomics intervention that successfully reduced agricultural [4] musculoskeletal disorders and poor posture can increase mental workload [15], increase risk perception and adoption of health behaviors, and promote a safe work environment [16], boosting general productivity [17] and job satisfaction [18].
Ergonomics in tourism trekking activities can be applied by (a) implementing a short break of 3 minutes every 1 hour of the journey, accompanied by a brief story about the surrounding natural environment during the break, and (b) providing information in the form of occupational health and safety (OHS) signs relating to danger warnings, evacuation routes, advisories and prohibitions. These measures aim to assess the reduction in fatigue and musculoskeletal disorders after implementing ergonomics in trekking activities. The hypothesis states that there are differences in fatigue and musculoskeletal disorders after applying ergonomics to trekking activities. The current research offered efforts to reduce complaints of fatigue and musculoskeletal disorders, as well as increased tourists’ satisfaction in Munduk Village, Bali.
II. LITERATURE REVIEW
A. Ergonomics Approach in Tourists Destinations
Ergonomics approach to tourism activities aims to modify the work environment, thereby improving working conditions, organization issues [19], and practices to reduce musculoskeletal disorders and fatigue [20]. Ergonomics (human factors engineering) approach to improving human performance [21] is related to various aspects, namely (1) Nutritional/energy needs [22], (2) Muscle power, including biomechanics, (3) Body posture/physiology, (4) Social/sociological conditions [23], (5) Work environment [24], (6) Working and rest time conditions [25] [26], (7) Information/interaction conditions of humans with visual displays [27], and (8) Human-machine interaction as a medium of transmission and exchange of information between workers and equipment [28].
B. Potential Dangers of Trekking Activities
Trekking activities, which are outdoor pursuits aimed at enjoying the panorama of nature and the environment over an extended and challenging period, can be carried out by anyone on foot with the aim of exploring nature for fun [29]. However, as trekking activities increase, tourists are often unaware of or unprepared for potential dangers. Factors such as lack of regulations and insufficient knowledge about disaster response can pose significant threat to tourists' safety [30]. The hazards associated with trekking activities often originate from continuous activities, including repetitive physical exertion, which can lead to fatigue or musculoskeletal disorders. To address these challenges, effective danger risk management is essential in tourism, as tourists may not always be adequately prepared to confront risk or hazard [31]. Engaging in outdoor recreational activities may increase the probability of encountering negative risk [32].
C. Complaints of Fatigue
Trekking is a physical activity that is carried out continuously, leading to fatigue as well as longer reaction times, reduced alertness, impaired memory, and impaired judgment, thereby decreasing occupational health [33]. Fatigue can be classified as follows [34]: (a). Physical fatigue, characterized by a significant decrease in mobility ability toward the end of the workday; (b). Mental fatigue, representing a decline in cognitive work ability toward the end of the work period; (c). Emotional labour burnout, reflecting a decrease in emotional activity toward the end of the workday.
D. Musculoskeletal Disorders
Musculoskeletal disorders refer to the onset of mild to very painful sensations in parts of the skeletal muscles experienced by individuals as a result of certain activities [35]. Continuous static work over extended periods can lead to damage in muscles, nerves, joints, ligaments, and tendons, resulting in complaints related to injuries in the skeletal muscle system, commonly known as musculoskeletal. disorders [36]. Musculoskeletal disorders can also originate from psychological mechanisms that induce stress, leading to muscle tension.
Increased psychological demands can amplify physical work demands and symptoms of musculoskeletal complaints [37]. These disorders are often associated with workplace conditions, characterized by repetitive movements over prolonged periods coupled with ergonomics work attitudes. Trekking as an activity of walking for extended periods, is often accompanied by unnatural body postures.
III. METHODS
A. Research Sites
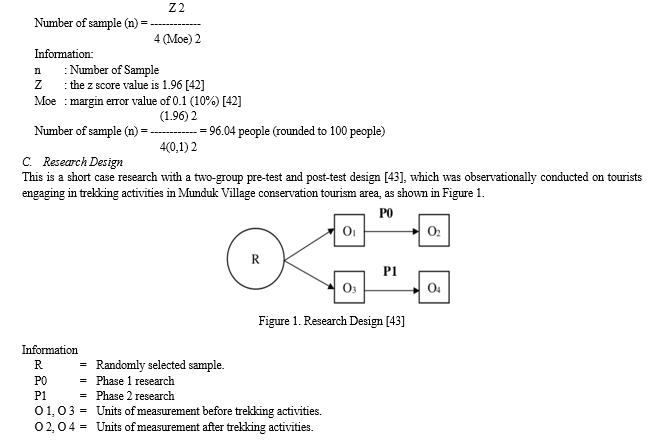
This research used a quantitative method, specifically a quasi-experimental two-group pre-test post-test control group design. The aim was to determine the effect of an intervention on an experimental group. This design offered a means of comparison between the two groups. Furthermore, it was conducted from July to September 2023 at the Munduk Village Trekking Tour, Banjar District, Buleleng Regency, passing three waterfalls, namely Melanting, Labuhan Kebo, and Red Coral.
B. Research Subject / Participants
The subjects were determined based on the following criteria: (a). Age range of 20-56 (b). Possessing a normal physique and ability to work without being hindered by physical limitations (c). Expressing willingness to participate as research subjects. Since the exact number of visiting tourists could not be determined, a Non-probability Sampling method was used [38] within the field of case-control research [39]. Accordingly, the sampled population should meet the specified criteria. The sampling technique used was Accidental Sampling [38] or convenience sampling with limited external validity [40]. Based on this method, the sample selection depended on the coincidence of meeting the research team. The sample size was calculated using the Slovin formula [41] due to the unlimited population.
D. Tasks and Assessment
Phase one research (P0) was conducted on 100 participants who met the inclusion criteria and expressed willingness to participate. Trekking activities were carried out according to established procedures without any ergonomics intervention. Phase two (P1) also included 100 participants who met the inclusion criteria and expressed willingness to participate. Trekking activities were carried out according to predetermined procedures and were accompanied by ergonomics intervention. This included implementing a short break of 3 minutes every hour of travel time and providing information/displays in the form of occupational health and safety (OHS) signs relating to danger warnings, evacuation routes, as well as warnings and prohibitions along trekking route. During the 3-minute breaks, participants were encouraged to relax and recover, and the tour guide provided a brief narrative about the surrounding natural environment.
Before commencing trekking activities in both phases, all participants had resting pulse recorded and completed musculoskeletal disorders and fatigue complaint questionnaires, assisted by the research team. The pulse rates were recorded every hour during trekking. After reaching the finish line, participants recorded recovery pulse rates and completed musculoskeletal disorders and fatigue complaint questionnaires, assisted by the research team. Musculoskeletal disorders were assessed using the Nordic Body Map questionnaire [44], while fatigue was evaluated using the EORTC Core questionnaire Quality of Life (EORTC QLQ-C30), designed to measure physical, psychological, and social functioning through multi-item and single-item scales [45]. After participating in the research activities, all participants received an appreciation note along with a souvenir, namely a 100-gram of locally sourced coffee powder from Tamblingan.
E. Research Procedure
The variables measured included: (1). Workload for trekking activities recorded from resting pulse (before starting activity) and working pulse (trekking activities recorded every hour); (2). Complaints of fatigue before and after trekking activities; (3). Musculoskeletal disorders before and after trekking activities. The variables were measured both before the implementation of ergonomics (P0) and after the implementation of ergonomics (P1).
F. Data Analysis
Collected data were analyzed through SPSS version 23.0, a statistical tool unraveling the intricate web of relationships among predetermined variables. The data comprising pulse rate, musculoskeletal complaints, and fatigue were meticulously scrutinized as follows: (1) Descriptive analysis showed the essence of the data's characteristics gleaned from research results; (2) The Shapiro-Wilk Test evaluated normality across all research data sets with a sample size less than 50; (3) Data comparability assessment juxtaposed pre-treatment (O1 and O3) and post-treatment (O2 and O4) average values; (4) Group data with a normal distribution underwent scrutiny through the Independent Sample Test; (5) Non-normally distributed data underwent transformation, and Wilcoxon Sign Ranks Test was conducted when normality was not achieved; (6) Treatment effect test, namely testing the difference in mean data after receiving treatment (O2 and O4); (7) A consistent significance level of 5% (α=0.05) showed the validity of all statistical examinations.
IV. RESULTS AND DISCUSSION
A. Participant Characteristics
This research included 100 participants in the control group (P0) and 100 in the treatment group (P1). The participants were tourists engaging in trekking activities from July to September 2023 at the Munduk Village Trekking Tour. The age range of those in the control group (P0) was between 24 and 55 years, with an average of 41.71 ± 9.95 years. The age for the treatment group (P1) ranged from 23 to 58 years, with an average of 41.91 ± 8.23 years. These ages fell within the working-age cohort and met the criteria for the labour force category as per BPS guidelines. The defined age range for Indonesia's labour force spans from 15 to 64 years, as mandated by the relevant legislation. The age range was consistent with musculoskeletal disorders research in fresh fruit bunch (FFB) harvesting processes with an average age of 25.4 ± 4.33 years [46], musculoskeletal disorders research in industrial workers comprising respondents aged 37 ± 8 years [47], and work posture research on truck manufacturing factory operators, with an average of 42.0 ± 7.6 years [48]. Trekking experience of participants in the control group (P0) was between 1-5 years with an average of 3.52 ± 1.38 years. Trekking experience of the treatment group (P1) participants was between 1-6 years, with an average of 3.27 ± 1.50 years. Further details are presented in Table 1.
Table 1. Descriptive statistics characteristics of control group (P0) and treatment group (P1) participants
|
Variables |
Group |
Descriptive Statistics |
||||
|
N |
Mean |
Minimum |
Maximum |
Standard Deviation |
||
|
Participant Age |
Control group (P0) |
100 |
41.71 |
24.00 |
55.00 |
7.95 |
|
Treatment group (P1) |
100 |
41.91 |
23.00 |
58.00 |
8.23 |
|
|
Trekking experience |
Control group (P0) |
100 |
3.52 |
1.00 |
5.00 |
1.38 |
|
Treatment group (P1) |
100 |
3.27 |
1.00 |
6.00 |
1.50 |
|
N: Number of participants
B. Trekking Activities Workload
Workload was assessed by measuring heart rate before and during trekking activities. The results showed that the average resting pulse rate of participants in the control group (P0) before trekking activities was 72.30 ± 3.99 beats/minute, with a minimum value of 64.00 beats/minute and a maximum of 78 beats/minute. In contrast, the average resting pulse rate of participants in the treatment group (P1) was 74.28 ± 5.12 beats/minute, with a minimum value of 64.00 beats/minute and a maximum of 80 beats/minute. The average pulse rate during trekking activities measured every hour in the control group (P0) was 114.57 ± 2.46 beats/minute, with a minimum of 108 beats/minute and a maximum of 122.00 beats/minute. Conversely, the average pulse rate during trekking activities in the treatment group (P1) was 107.73 ± 2.68 beats/minute, with a minimum of 96.00 beats/minute and a maximum 114.00 beats/minute. Further details are presented in Table 3.
Table 3. Descriptive statistics resting pulse rate and pulse rate during trekking activities of control group (P0) and treatment group (P1) participants
|
Variables |
Group |
Descriptive Statistics |
||||
|
N |
Mean |
Minimum |
Maximum |
Standard Deviation |
||
|
Resting pulse before trekking activities |
Control group (P0) |
100 |
72.30 |
64.00 |
78.00 |
3.99 |
|
Treatment group (P1) |
100 |
74.28 |
64.00 |
80.00 |
5.12 |
|
|
The pulse of trekking activity |
Control group (P0) |
100 |
114.57 |
108.00 |
122.00 |
2.46 |
|
Treatment group (P1) |
100 |
107.73 |
96.00 |
114.00 |
2.68 |
|
N: Number of participants
The average pulse rate during trekking activities for the control group (P0) was 114.57 ± 2.46 beats/minute, while the average pulse rate for the treatment group (P1) was 107.73 ± 2.68 beats/minute, showing a difference in heart rate. The pulse of participants in the treatment group (P1) was lower than that of the control group (P0). Therefore, the treatment effect of applying ergonomics to trekking activities could reduce workload (activities pulse) by 5.97%. Kolmogorov-Smirnov test results for resting pulse rate before and during trekking activities and pulse rate in both the control group (P0) and treatment group (P1) were (p >0.05), showing normal distribution of data. Independent sample test showed that the average resting pulse rate before trekking activities between the control group (P0) and the treatment group (P1) was not significantly different, (p > 0.05), with similar influence in both groups. However, the independent sample test for the average pulse rate showed a significant difference between the control group (P0) and treatment group (P1) (p < 0.05). The treatment effect of applying ergonomics to the treatment group's trekking activities influenced a reduction in workload during activities. Several research provided evidence regarding the effectiveness of alternative approaches to ergonomics intervention, such as process-oriented ergonomics, which could address some of the more complex aspects of human-machine-environment interactions [49]. This was consistent with research showing a relationship between physical tasks, cognitive, manual control, and time pressure, and the subjective burden experienced by an operator [50]. The results of the independent sample test are presented in Table 4.
Table 4. Kolmogorov-Smirnov test and independent sample test average resting pulse rate and trekking activities pulse rate of control group (P0) and treatment group (P1) participants
|
Variables |
Group |
N |
Kolmogorov-Smirnov Test |
Independent Sample Test |
|
|
p |
t |
p |
|||
|
Resting pulse before trekking activities |
Control group (P0) |
100 |
0.068 |
-3,046 |
0.013 |
|
Treatment group (P1) |
100 |
0.114 |
|||
|
The pulse of trekking activities |
Control group (P0) |
100 |
0.110 |
18,788 |
0,000 |
|
Treatment group (P1) |
100 |
0.152 |
|||
N: Number of participants
C. Complaints of Fatigue
Fatigue complaints were measured based on general fatigue experienced before and after trekking activities. Feelings of fatigue were measured by completing the EORTC Core questionnaire Quality of Life (EORTC QLQ-C30) independently. The results showed that the average fatigue complaint score before trekking activities in the control group (P0) was 31.52 ± 0.99, with a minimum score of 30.00 and a maximum of 33.00. The average fatigue score before trekking activities in the treatment group was 30.60 ± 1.06, with a minimum of 29.00 and a maximum of 32.00. The average fatigue score after trekking activities in the control group (P0) was 45.60 ± - 3.04, with a minimum of 39.00 and a maximum of 51.00. The average fatigue score after trekking activities in the treatment group (P1) was 40.51 ± 2.89, with a minimum of 37.00 and a maximum of 43.00. The increase in fatigue score after trekking activities was 44.67% in the control group (P0) and 32.38% in the treatment group (P1). The results were consistent with research showing that implementing simple, practical improvements applying basic ergonomics principles reduced work-related risk [51] [52]. Fatigue complaint scores are presented in Table 5.
Table 5. Descriptive statistics on fatigue scores before and after trekking activities of control group (P0) and treatment group (P1) participants
|
Variables |
Group |
Descriptive Statistics |
||||
|
N |
Mean |
Minimum |
Maximum |
Standard Deviation |
||
|
Fatigue before trekking activities |
Control group (P0) |
100 |
31.52 |
30.00 |
33.00 |
0.99 |
|
Treatment group (P1) |
100 |
30.60 |
29.00 |
32.00 |
1.06 |
|
|
Fatigue after trekking activities |
Control group (P0) |
100 |
45.60 |
39.00 |
51.00 |
3.04 |
|
Treatment group (P1) |
100 |
40.51 |
37.00 |
43.00 |
2.89 |
|
Kolmogorov-Smirnov results for fatigue complaint before trekking activities in both the control group (P0) and treatment group (P1) were p >0.05, showing normal distribution of data. Independent sample test showed the average fatigue complaint scores before trekking activities between the control group (P0) and the treatment group (P1) were not significantly different (p > 0.05). The average fatigue complaint score before trekking activities had a similar influence on trekking activities in both groups. However, independent sample test for the average complaint score during trekking activities showed a significant difference between the control group (P0) and the treatment group (P1) (p < 0.05). This showed that the treatment effect of applying ergonomics to the treatment group (P1) trekking activities had an influence on reducing fatigue complaint score during trekking activities. The results of the independent sample test are presented in Table 6.
Table 6. Kolmogorov-Smirnov test and independent sample test average score complaints of fatigue before and after trekking activities of control group (P0) and treatment group (P1) participants
|
Variables |
Group |
N |
Kolmogorov-Smirnov Test |
Independent Sample Test |
|
|
p |
t |
p |
|||
|
Complaint Score Fatigue before trekking activities |
Control group (P0) |
100 |
0.410 |
6,302 |
0.010 |
|
Treatment group (P1) |
100 |
0.087 |
|||
|
Complaint Score Fatigue after trekking activities |
Control group (P0) |
100 |
0.068 |
4,975 |
0,000 |
|
Treatment group (P1) |
100 |
0.090 |
|||
D. Musculoskeletal Disorders
Musculoskeletal disorders were measured based on the complaints felt by participants before and after trekking activities. Participants' perception of musculoskeletal disorders was measured by completing the Nordic Body Map questionnaires independently. The results showed that musculoskeletal disorders score before trekking activities in the control group (P0) was 29.93 ± 0.75, with a minimum of 29.00 and maximum of 32.00. The average score before trekking activities in the treatment group (P1) was 29.66 ± 1.53, with a minimum of 28.00 and a maximum of 32.00. The average musculoskeletal disorders score after trekking activities in the control group (P0) was 51.87 ± 5.77, with a minimum of 39.00 and a maximum of 66.00. The average score in the treatment group (P1) was 43.34 ± 5.38, with a minimum of 37.00 and a maximum of 61.00. The improvement in musculoskeletal disorders score after trekking activities in the control group (P0) was 73.30% and 46.12% in the treatment group (P1). This increase could be attributed to the repetitive movements and prolonged static postures during trekking activities, leading to muscle tension and increased stress levels [37]. Prolonged static movements can also cause damage to muscles, nerves, joints, ligaments and tendons, contributing to musculoskeletal disorders [53], [54].
Table 7. Descriptive statistics musculoskeletal score disorders before and after trekking activities of control group (P0) and treatment group (P1) participants
|
Variables |
Group |
Descriptive Statistics |
||||
|
N |
Mean |
Minimum |
Maximum |
Standard Deviation |
||
|
Musculoskeletal scores? disorders before trekking activities |
Control group (P0) |
100 |
29.93 |
29.00 |
32.00 |
0.75 |
|
Treatment group (P1) |
100 |
29.66 |
28.00 |
32.00 |
1.53 |
|
|
Musculoskeletal scores? disorders after trekking activities |
Control group (P0) |
100 |
51.87 |
39.00 |
66.00 |
5.77 |
|
Treatment group (P1) |
100 |
43.34 |
37.00 |
61.00 |
5.38 |
|
N: Number of participants
Kolmogorov-Smirnov test results for musculoskeletal disorders score before trekking activities in both the control group (P0) and treatment group (P1) were p >0.05, showing normal distribution of data. Independent sample test showed that the average musculoskeletal disorders score before trekking activities between the control group (P0) and the treatment group (P1) was not significantly different (p > 0.05), with both groups having similar influence. Independent sample test for the average musculoskeletal disorders score between the control group (P0) and treatment group (P1) was significantly different (p < 0.05). This showed that the treatment effect of applying ergonomics to the treatment group's trekking activities influenced a reduction in musculoskeletal disorders scores during trekking activities. The results of independent sample test are presented in Table 8.
Table 8. Kolmogorov-Smirnov test and Independent Sample test average musculoskeletal ? disorders scores before and after trekking activities of control group (P0) and treatment group (P1) participants
|
Variables |
Group |
N |
Kolmogorov-Smirnov Test |
Independent Sample Test |
|
|
p |
t |
p |
|||
|
Musculoskeletal disorders scores before trekking activities |
Control group (P0) |
100 |
0.019 |
1,580 |
0.116 |
|
Treatment group (P1) |
100 |
0.176 |
|||
|
Musculoskeletal disorders scores after trekking activities |
Control group (P0) |
100 |
0.200 |
3,205 |
0.002 |
|
Treatment group (P1) |
100 |
0.514 |
|||
N: Number of participants
V. ACKNOWLEDGMENT
The authors are grateful to the Ministry of Education, Culture, Research and Technology of Indonesia, through the Directorate General of Vocational Education for funding the PIPK Smart Village Program Munduk Tourism Village Using the Ergo-Infocom Approach for Economic Recovery Due to the Covid-19 Pandemic, in 2022-2023. The authors also acknowledge the funding received for the Matching Fund Program "Development of Conservation Tourism in Munduk Village Area Through an Ergonomics Approach" in 2023.
Conclusion
In conclusion, ergonomics intervention was provided to tourists engaging in trekking activities for 4 hours in Munduk Village Trekking Tour, Banjar District, Buleleng Regency, passing through three waterfalls, namely Melanting, Labuhan Kebo, and Red Coral. This included implementing short breaks of 3 minutes for relaxation and recovery, providing narratives about the surrounding natural environment every hour during trekking activities, offering information/displays in the form of occupational health and safety (OHS) signs related to danger warnings, evacuation routes, and prohibitions along the route. The intervention had a significant effect on reducing pulse rate during trekking and alleviating fatigue as well as musculoskeletal disorders. Ergonomics strategies aimed to prevent increased fatigue after work by optimizing task duration and training levels [55], and by relating human factors with work systems and environmental conditions to meet human needs, abilities, and limitations [56], [57]. Furthermore, implementing technical and organizational ergonomics intervention could help reduce physical workloads [48], while the application of total ergonomics included designing work systems considering human, environmental, and organizational factors within the production system [58],[59], [60].
References
[1] Y. Zou and Q. Yu, “Sense of safety toward tourism destinations: A social constructivist perspective,” Journal of Destination Marketing and Management, vol. 24, June. 2022, doi: 10.1016/j.jdmm.2022.100708. [2] International Labour Organization, “The future of work in the tourism sector: Sustainable and safe recovery and decent work in the context of the COVID-19 pandemic Report for the Technical Meeting on COVID-19 and Sustainable Recovery in the Tourism Sector,” Geneva, Apr. 2022. Accessed: Feb. 18, 2024. [Online]. Available: https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---sector/documents/meetingdocument /wcms_840403.pdf [3] A. Garg, “Travel Risks vs Tourist Decision Making: A Tourist Perspective,” International Journal of Hospitality & Tourism Systems, vol. 8, no. 1, June. 2021, DOI: 10.21863/ ijhts /2015.8.1.004. [4] A. Jirapongsuwan, P. Klainin-Yobas, W. Songkham, S. Somboon, N. Pumsopa, and P. Bhatarasakoon, “The effectiveness of ergonomic intervention for preventing work-related musculoskeletal disorders in agricultural workers: A systematic review protocols,” PLoS One, vol. 18, no. 7 July, Jul. 2023, doi: 10.1371/journal.pone.0288131. [5] J. Yin, Y. Ji, P. Huang, and Y. Ni, “Fatigue or satisfaction at crowded attractions?,” Current Psychology, vol. 42, no. 36, pp. 32588–32599, Dec. 2023, doi: 10.1007/s12144-023-04263-3. [6] C.E. Izard, “Basic Emotions, Natural Kinds, Emotion Schemas, and a New Paradigm,” Perspectives on Psychological Science, vol. 2, no. 3, pp. 260–280, Sept. 2007, doi:10.1111/j.1745-6916.2007.00044.x. [7] N. Ali Alzahrani, \"Workplace Ergonomics and Academic Staff Performance in College of Education in Umm Al- Qura University in Makkah,\"American Journal of Educational Research”, vol. 7, no. 9, pp. 604–617, Sept. 2019, doi: 10.12691/education-7-9-2. [8] PR Fernandes, ALB Hurtado, and EC Batiz, “Ergonomics Management with a Proactive Focus,” Procedia Manufacturing, vol. 3, pp. 4509–4516, 2015, doi:10.1016/j.promfg.2015.07.465. [9] Robert L. Getty, “Quality and Ergonomics: Application of Ergonomics to Continuous Improvement Is Integral to the Goals of Business,” in Occupational Ergonomics: Design and Management of Work Systems, 1st ed., vol. 1, Waldemar Karwowski; William S. Marras, Ed., New York: CRC Press, Boca Raton, 2003, pp. 1–16. [10] JN Ugbebor and SS Adaramola, “Evaluating the effectiveness of ergonomics applications,” in Work, 2012, pp. 484–486. doi: 10.3233/WOR-2012-0200-484. [11] A. Padhil and H. Purnomo, \" Macroergonomic approaches as a solution to local wisdom-based tourist village development planning,\" MATEC Web of Conferences, vol. 154, p. 01080, Feb. 2018, doi: 10.1051/ matecconf /201815401080. [12] R. Robina-Ramírez, R. Ravina -Ripoll, and F.J. Castellano-Álvarez, “The trinomial of health, safety and happiness promotes rural tourism,” BMC Public Health, vol. 23, no. 1, Dec. 2023, doi: 10.1186/s12889-023-15849-8. [13] C. Wife Dharmayanti, A. Ayu Biomi, and Marniati, \"Analysis of Security and Safety of Tourists at Waterfalls in Gianyar Regency,\" PROMOTOR: Public Health Student Journal, vol. 6, no. 5, pp. 476–480, 2023, doi: 10.32832/pro. [14] A. Singh and VK Singh, “The impact of ergonomic practices on housekeeping employee retention and efficiency in hotels during COVID-19 in India,” Turyzm /Tourism, vol. 32, no. 2, pp. 29–50, 2022, doi: 10.18778/0867-5856.32.2.02. [15] V. Nino, D. Claudio, and S. M. Monfort, “Evaluating the effect of perceived mental workload on work body postures,” International Journal of Industrial Ergonomics, vol. 93, Jan. 2023, doi: 10.1016/j.ergon.2022.103399. [16] S. Yang, L. Li, L. Wang, J. Zeng, B. Yan, and Y. Li, “Effectiveness of a multidimensional intervention program in improving occupational musculoskeletal disorders among intensive care unit nurses: a cluster-controlled trial with follow-up at 3 and 6 months,” BMC Nurs, vol. 20, no. 1, Dec. 2021, doi: 10.1186/s12912-021-00561-y. [17] HMMM Jayawickrama, M. Dharmawardana, AK Kulatunga, KGSP Karunarathna, and SAU Osadith, “Enhancement of Productivity of Traditional Brass Manufacturing Industry Using Sustainable Manufacturing Concept,” Procedia CIRP, vol. 40, pp. 562–567, 2016, doi: 10.1016/j.procir.2016.01.134. [18] N. Ali Alzahrani, \"Workplace Ergonomics and Academic Staff Performance in College of Education in Umm Al-Qura University in Makkah,\" American Journal of Educational Research, vol. 7, no. 9, pp. 604–617, 2019, doi: 10.12691/education-7-9-2. [19] Meyer F, Eweje G, and Tappin D, “Ergonomics as a tool to improve the sustainability of the workforce,” Work, vol. 57, no. 3, pp. 339–350, 2017. [20] García AM, Boix P, G Benavides F, Gadea R, Rodrigo F, and Serra C, “Participación para mejorar las condiciones de trabajo: evidencias y experiencias [Participation to improve working conditions: evidence and experience],” Gac Sanit, vol. 30, no. 1, pp. 87–92, Nov. 2016, doi: 10.1016/j.gaceta.2016.03.006. [21] SJ Guastello, Human Factors Engineering and Ergonomics A Systems Approach, Second. 6000 Broken Sound Parkway NW, Suite 300 Boca Raton, FL 33487-2742: CRC Press Taylor & Francis Group, 2014. Accessed: Jul. 27, 2023. [Online]. Available: https://industri.fatek.unpatti.ac.id/wp-content/uploads/2019/03/102-Human-Factors-Engineering-and-Ergonomics-A-Systems-Approach-Stephen-J.-Guastello -Edition-2-2013.pdf [22] Bijetri Bandyopadhyay and Devashish Sen, “Assessment of energy balance against the nutritional status of women carriers in the brickfields of West Bengal,” International Journal of Occupational Safety and Ergonomics, vol. 2, no. 3, pp. 339–404, Apr. 2016, DOI: 10.1080/10803548.2016.1165529. [23] J. Shearer, T. E. Graham, and T. L. Skinner, “Nutra-ergonomics: influence of nutrition on physical employment standards and the health of workers,” Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolism, vol. 41, no. 6. pp. S165–S174, Jun. 01, 2016. doi: 10.1139/apnm-2015-0531. [24] ZKM Makhbul, MS Shukor, and AA Muhamed, “Ergonomics workstation environment toward organizational competitiveness,” International Journal of Public Health Science, vol. 11, no. 1, pp. 157–169, March. 2022, doi: 10.11591/ijphs.v11i1.20680. [25] Cheng-Lung Lee, Shih-Yi Lu, and Chang-You Wu, “Rest period and object load effects on upper limb muscle strength recovery for manual load transfer,” International Journal of Industrial Ergonomics, vol. 89, May 2022, Accessed: Jul. 27, 2023. [Online]. Available: https://doi.org/10.1016/j.ergon.2022.103274 [26] Dias NF, Tirloni AS, Cunha Dos Reis D, and Moro ARP, “The effect of different work-rest schedules on ergonomic risk in poultry slaughterhouse workers,” Work, vol. 69, no. 1, pp. 215–223, 2021, DOI: 10.3233/WOR-213471. [27] Martina Ziefle, “Visual Ergonomic Issues of LCD Displays – An Insight into Working Conditions and User Characteristics,” in Industrial Engineering and Ergonomics, 2009. DOI: 10.1007/978-3-642-01293-8_41. [28] MC Edith, EE Obiageli, OC Chikwendu, and MC Ogonna, “Man-Machine Systems: A Review of Current Trends and Applications,” FUPRE Journal of Scientific and Industrial Research, vol. 4, no. 2, pp. 91–117, 2020. [29] dr. Rizal Fadli, \" Getting to Know the Differences between Hiking and Trekking Sports and Benefits,\" https://www.halodoc.com/article/mengenal-beda-olahraga-hiking-dan-trekking-and-tidaknya#:~:text=2.%20Trekking, exploring%20nature%20by%20walking%20foot. [30] Y. Mu and S. Nepal, “High Mountain Adventure Tourism: Trekkers\' Perceptions of Risk and Death in Mt. Everest Region, Nepal,” Asia Pacific Journal of Tourism Research, vol. 21, no. 5, pp. 500–511, May 2016, doi: 10.1080/10941665.2015.1062787. [31] A.D. Ziegler et al., “A call for reducing tourism risk to environmental hazards in the Himalayas,” Environmental Hazards, vol. 22, no. 1, pp. 1–28, Jan. 2023, doi: 10.1080/17477891.2021.1984196. [32] A. M. Gstaettner, D. Lee, and K. Rodger, “The concept of risk in nature-based tourism and recreation – a systematic literature review,” Current Issues in Tourism, vol. 21, no. 15, pp. 1784–1809, Oct. 2018, doi: 10.1080/13683500.2016.1244174. [33] The National Institute for Occupational Safety and Health (NIOSH), “Work and Fatigue,”https://www.cdc.gov/niosh/topics/fatigue/default.html#:~:text=Fatigue%20has% 20been%20described%20as,work%20and%20extended%20work%20hours. [34] MR Frone and MCO Tidwell, “The meaning and measurement of work fatigue: Development and evaluation of the three-dimensional work fatigue inventory (3d-wfi),” Journal of Occupational Health Psychology, vol. 20, no. 3, pp. 273–288, Jan. 2015, doi: 10.1037/a0038700. [35] S. Mohamaddan et al., “Investigation of oil palm harvesting tools design and technique on work-related musculoskeletal disorders of the upper body,” International Journal of Industrial Ergonomics, vol. 86, Nov. 2021, doi: 10.1016/j.ergon.2021.103226. [36] L. Tang, G. Wang, W. Zhang, and J. Zhou, “The prevalence of MSDs and the associated risk factors in nurses of China,” International Journal of Industrial Ergonomics, vol. 87, Jan. 2022, doi: 10.1016/j.ergon.2021.103239. [37] L. Mateos -Gonzalez, J. Rodríguez-Suárez, and J. A. Llosa, “A systematic review of the association between job insecurity and work-related musculoskeletal disorders,” Human Factors and Ergonomics in Manufacturing, vol. 34, no. 2. John Wiley and Sons Inc, pp. 79–99, March. 01, 2024. doi: 10.1002/hfm.21013. [38] A.E. Berndt, “Sampling Methods,” Journal of Human Lactation, vol. 36, no. 2, pp. 224–226, May 2020, doi: 10.1177/0890334420906850. [39] KS Kim, “Methodology of Non-probability Sampling in Survey Research,” American Journal of Biomedical Science and Research, vol. 15, no. 6, pp. 616–618, March. 2022, doi: 10.34297/ajbsr.2022.15.002166. [40] C. Andrade, “The Inconvenient Truth About Convenience and Purposive Samples,” Indian Journal of Psychological Medicine, vol. 43, no. 1, pp. 86–88, Jan. 2021, doi: 10.1177/0253717620977000. [41] J. J. Tejada, J. Raymond, and B. Punzalan, “On the Misuse of Slovin\'s Formula,” The Philippine Statistician, vol. 61, no. 1, pp. 129–136, 2012, Accessed: June. 25, 2023. [Online]. Available: https://www.psai.ph/docs/publications/tps/tps_2012_61_1_9.pdf [42] A. Althubaiti, “Sample size determination: A practical guide for health researchers,” Journal of General and Family Medicine, vol. 24, no. 2. John Wiley and Sons Inc, pp. 72–78, March. 01, 2023. doi: 10.1002/jgf2.600. [43] MN Marshall, “Sampling for qualitative research,” 1996. [Online]. Available: https://academic.oup.com/fampra/article/13/6/522/496701 [44] KJI Kuorinka, B. Jonsson, A. Kilbom, H. Vinterberg, F. Biering-Sørensen, G. Andersson, “Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms,” Applied Ergonomics, vol. 18, no. 3, pp. 233–237, 1987, Accessed: June. 22, 2023. [Online]. Available: https://doi.org/10.1016/0003-6870(87)90010-X [45] A. Penson et al., “Short fatigue questionnaire: Screening for severe fatigue.,” Journal of Psychosomatic Research, vol. 137, Oct. 2020, doi: 10.1016/j.jpsychores.2020.110229. [46] S. Mohamaddan et al., “Investigation of oil palm harvesting tools design and technique on work-related musculoskeletal disorders of the upper body,” International Journal of Industrial Ergonomics, vol. 86, Nov. 2021, doi: 10.1016/j.ergon.2021.103226. [47] AS Oestergaard, TF Smidt, K. Søgaard, and LF Sandal, “Musculoskeletal disorders and perceived physical work demands among offshore wind industry technicians across different turbine sizes: A cross-sectional study,” International Journal of Industrial Ergonomics, vol. 88, March. 2022, doi: 10.1016/j.ergon.2022.103278. [48] M. Zare, N. Black, J.C. Sagot, G. Hunault, and Y. Roquelaure, “Ergonomics interventions to reduce musculoskeletal risk factors in a truck manufacturing plant,” International Journal of Industrial Ergonomics, vol. 75, Jan. 2020, doi: 10.1016/j.ergon.2019.102896. [49] T. Engström, A. Portolomeos, L. Hanson, L. Medbo, and R. Akselsson, “Process Oriented Ergonomics – The Ergonomics of the Future? A Case Study of Integrated Ergonomics at an Engine Assembly Plant,” Proceedings of the Human Factors and Ergonomics Society Annual Meeting, vol. 44, no. 29, pp. 328–331, Jul. 2000, doi: 10.1177/154193120004402986. [50] N. Moray, “Subjective Mental Workload,” Human Factors: The Journal of the Human Factors and Ergonomics Society, vol. 24, no. 1, pp. 25–40, Feb. 1982, doi: 10.1177/001872088202400104. [51] K. Kogi, “Practical Ways to Facilitate Ergonomics Improvements in Occupational Health Practice,” Human Factors: The Journal of the Human Factors and Ergonomics Society, vol. 54, no. 6, pp. 890–900, Dec. 2012, doi: 10.1177/0018720812456204. [52] P. Rodrigues Armijo, C.-K. Huang, T. Carlson, D. Oleynikov, and K.-C. Siu, “Ergonomics Analysis for Subjective and Objective Fatigue Between Laparoscopic and Robotic Surgical Skills Practice Among Surgeons,” Surgical Innovation, vol. 27, no. 1, pp. 81–87, Feb. 2020, doi: 10.1177/1553350619887861. [53] G. Kar and A. Hedge, “Effects of a sit-stand-walk intervention on musculoskeletal discomfort, productivity, and perceived physical and mental fatigue, for computer-based work,” International Journal of Industrial Ergonomics, vol. 78, Jul. 2020, doi: 10.1016/j.ergon.2020.102983. [54] A. Choobineh et al., “A multilayered ergonomic intervention program on reducing musculoskeletal disorders in an industrial complex: A dynamic participatory approach,” International Journal of Industrial Ergonomics, vol. 86, Nov. 2021, doi: 10.1016/j.ergon.2021.103221. [55] P. Rodrigues Armijo, C.-K. Huang, T. Carlson, D. Oleynikov, and K.-C. Siu, “Ergonomics Analysis for Subjective and Objective Fatigue Between Laparoscopic and Robotic Surgical Skills Practice Among Surgeons,” Surgical Innovation, vol. 27, no. 1, pp. 81–87, Feb. 2020, doi: 10.1177/1553350619887861. [56] W. Karwowski and W.S. Marras, “Occupational Ergonomics: Design and Management of Work Systems,” Boca Raton New York, 2003. Accessed: Jul. 27, 2023. [Online]. Available: https://ftp.idu.ac.id/wp-content/uploads/ebook/ip/Buku%20ergonomi/Buku%20inggris/Occupational%20Ergonomics%20Design%20and%20Managementof%20Work%20Systems.pdf [57] Kageyu Noro, “Participatory Ergonomics,” in Occupational Ergonomics: Design and Management of Work Systems, Waldemar Karwowski and William S. Marras, Eds., Boca Raton New York: CRC Press, 2003, pp. 1–9. Accessed: Jul. 27, 2023. [Online]. Available: https://ftp.idu.ac.id/wp-content/uploads/ebook/ip/Buku%20ergonomi/Buku%20inggris/Occupational%20Ergonomics%20Design%20and%20Managementof%20Work%20Systems.pdf [58] S.E. Peters, H.D. Trieu, J. Manjourides, J.N. Katz, and J.T. Dennerlein, “Designing a participatory total worker health® organizational intervention for commercial construction subcontractors to improve worker safety, health, and well-being: The \'arm for subs\' trial,” International Journal of Environmental Research and Public Health, vol. 17, no. 14, pp. 1–15, Jul. 2020, doi: 10.3390/ijerph17145093. [59] A. Manuaba, “Total Approach is a Must for Small and Medium Enterprises to Attain Sustainable Working Conditions and Environment, with Special Reference to Bali, Indonesia,” Industrial Health, vol. 44, pp. 22–26, 2006. [60] H. Sajiyo, A. Manuaba, N. Adiputra, and P. Sutjana, “Redesign Of Work Place And System With Ergonomic Intervention Improves The Performance Of The Skt (Hand Rolled Cigarette) Rollers At Cigarette Industry €Œxâ €& #157; In Kediri East Java,\" Indonesian Journal of Biomedical Science, vol. 3, no. 1, Nov. 2012, doi: 10.15562/ijbs.v3i1.61.
Copyright
Copyright © 2024 I Ketut Gde Juli Suarbawa, M. Yusuf, Lilik Sudiajeng. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Download Paper
Paper Id : IJRASET63099
Publish Date : 2024-06-04
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here
 Submit Paper Online
Submit Paper Online