

Ijraset Journal For Research in Applied Science and Engineering Technology
Design and Development of Automated Lower Limb Continuous Passive Motion (CPM) Machine
Authors: Prof. Manish Dakhore, Navneet Shelke , Samyak Meshram, Yash Kuhikar
DOI Link: https://doi.org/10.22214/ijraset.2024.62407
Certificate: View Certificate
Abstract
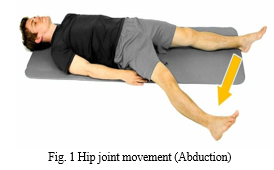
Post-operative rehabilitation is critical in orthopedic surgery, especially for hip joint surgeries. Traditional therapies like manual exercises and resource limits in rehabilitation centers might be tough, but early mobilization and rehabilitation are critical for regaining joint function and allowing patient return to normal activities. Continuously Passive Motion (CPM) devices, primarily developed for knee joint rehabilitation, offer a non-invasive method for passive joint mobility, restoring joint range of motion and lowering post-operative stiffness risk. Their application in hip joint healing is gaining pace, offering better results and increased patient satisfaction. The research also investigates abduction mobility in the hip joint, which is necessary for daily actions like stepping to the side, getting out of bed, or exiting a car. Understanding hip joint biomechanics and range of motion parameters is vital for establishing efficient rehabilitation approaches. By merging clinical insights with technology innovations, this research intends to optimize post-surgery rehabilitation regimens, enhancing patient outcomes and quality of life. The subject of orthopedic rehabilitation continues to expand through interdisciplinary collaboration and innovation, bringing new choices for enhancing patient care and recovery trajectories.
Introduction
I. INTRODUCTION
After surgery, joint pain and stiffness might arise, impairing the patient's ability to touch or move their limb. Rehabilitation is necessary everyday for 4-6 months, depending on the severity of the fracture. The hip joint, a ball and socket joint, is vital for bearing bodyweight and executing movement. Physical rehabilitation strives to preserve, restore, and develop human body movement through physical therapy[1].
Physiotherapists give rehabilitation exercises, manipulating the joint without the patient's muscles being utilized. Active exercises are performed by the patient without resistance, and the last phase of therapy can be began with resistive exercises focusing on enhancing proprioceptive abilities through walking. Hip rehabilitation therapy is a protracted process that includes manual exercises, time, and patience.
However, physical motions for hip-joint rehabilitation are strenuous, and session time is usually regulated by the physiotherapist[12][18].
Continuous passive motion machines (CPM) are often used following joint surgery to enhance recovery of normal joint range of motion (ROM) and minimize joint stiffness problems. CPM machines are most typically applied to the knee but have equivalents for other joints such as the hip, shoulder, and elbow. Abduction movement is a regular daily action, with a maximum permitted motion of 45 degrees[11][2]. A literature analysis and market survey indicated that there is no mechanism available for supplying continuous passive motion to the hip joint.
Therefore, there is scope to design and create an automated system for the lower limb of the hip joint[8]. The problem statement is that the abduction movement is now done manually by a physiotherapist, which costs money, time, and inconveniences the patient. An automated method might make this process straightforward and easy, making it more cost-effective and convenient for patients and experts[22][23][3].
The aims of this project are to automate the continuous passive motion for the lower leg, offer the patient with continuous passive motion, construct a user-friendly device, provide changeable settings, and enhance patient comfort and overall experience.
II. LITERATURE SURVEY
The review of the literature offers a complete overview of the design and manufacture of an automated lower limb continuous passive motion system. The study focuses on the efficiency of continuous passive motion (CPM) rehabilitation in restoring joint amplitude, enhancing muscle tissue excitability and trophicity, and preventing immobilization edema[8][9]. The research also addresses the reliability of physical examination in measuring hip range of motion (ROM) and the reliability of manual versus computerized procedures for assessing passive stiffness of posterior muscles of the hip and thigh[3].
The addresses the design and robust motion control of a planar 1P-2P RP hybrid manipulator for lower limb rehabilitation applications. [12] The paper also describes the rehabilitation process and how CPM devices are utilized to restore joint mobility and function. The paper also examines the fast-track procedure for hip and knee arthroplasty, including multimodal pain treatment, early mobilization, and functional discharge criteria[8].
To examines ways for preventing capsulolabral adhesions after hip arthroscopy, which can weaken the labrum. The study also introduces a simple hip-joint rehabilitation robot (HipBot) built to conduct combined movements of abduction/adduction and flexion/extension. The study concludes that continuous passive motion machines can be used as an addition to conventional physiotherapy following hemiarthroplasty[22].
The use of physiotherapy in peri-operative treatment in total knee and hip surgery is critical for superior functional outcomes. Preoperative or post-operative physical therapy offers great benefits in terms of pain tolerance and speedier rehabilitation[19]. Post-operative guidelines following hip arthroscopy should be followed, with doctors acknowledging the need to evaluate joint mobility after each loading event and noting that there will be a soft tissue adjustment period following FAI surgery[6][1].
Several research have addressed the development of innovative rehabilitation equipment for the recovery of lower limb bearing joints, such as pneumatic muscle actuators for continuous passive motion (CPM) rehabilitation. These devices have been demonstrated useful in restoring joint amplitude, enhancing muscle tissue excitability and trophicity, and reducing immobilization edema.
A control method for a hip-joint rehabilitation robot based on Generalized Proportional Integral (GPI) controllers has been developed, seeking to guarantee trajectory tracking during rehabilitation while rejecting unexpected disturbances and dynamic changes. The results indicate the GPI controllers' capacity to follow planned trajectories despite noisy readings and dynamic changes from changing patient weights[13].
Using an isokinetic dynamometer, a study comparing the accuracy of a manual and automated technique for assessing the passive stiffness of posterior thigh muscles revealed that both methods were equally reliable for measuring passive stiffness throughout the range of motion[14].
A planar 1P-2PRP hybrid manipulator for lower limb rehabilitation applications has been designed and developed, with three degrees of freedom in the sagittal plane and operating with a passive leg orthosis. The device's usefulness is tested experimentally on a prototype utilizing a clinical gait pattern[25].
F. AutoCAD 2016 Software
A virtual model of a continuous passive motion machine is designed using AutoCAD 2016 software. The menu bar, drawing area, several toolbars, command window, model and layout tabs, and status bar are some of the elements that make up the standard AutoCAD screen[13]. The name of the active drawing appears at the top of the screen, and there is an AutoCAD symbol in the title bar.
In 2D or 3D, AutoCAD offers the greatest drafting and design capabilities available. With capabilities to create plan, elevation, and isometric views automatically, tool palettes to store your favorite blocks, and machine learning tools to teach you new design techniques, AutoCAD offers an unparalleled user experience that millions of users worldwide rely on.Compared to other CAD alternatives, the dwg file format from Autodesk offers the most accurate and efficient means of viewing and editing DWGs. [12]When utilizing other products, users have reported a higher risk of faulty data, delays in importing and exporting files, missing items, and poor conversion quality.
G. Software for Arduino IDE
Arduino microcontroller boards are programmed using the Arduino IDE (Integrated Development Environment). It offers an easy-to-use interface for creating, gathering, and uploading code to Arduino hardware. Because of its streamlined programming language, which is based on C/C++, users may simply construct interactive electronic creations. To test code before uploading it, the Arduino IDE comes with a text editor, a compiler, and an augmented reality version of the Arduino board. Because it is open-source, it can be customized extensively and has community assistance, making it useful for both novice and seasoned embedded systems and electronics developers[11].
V. WORKING OF SYSTEM
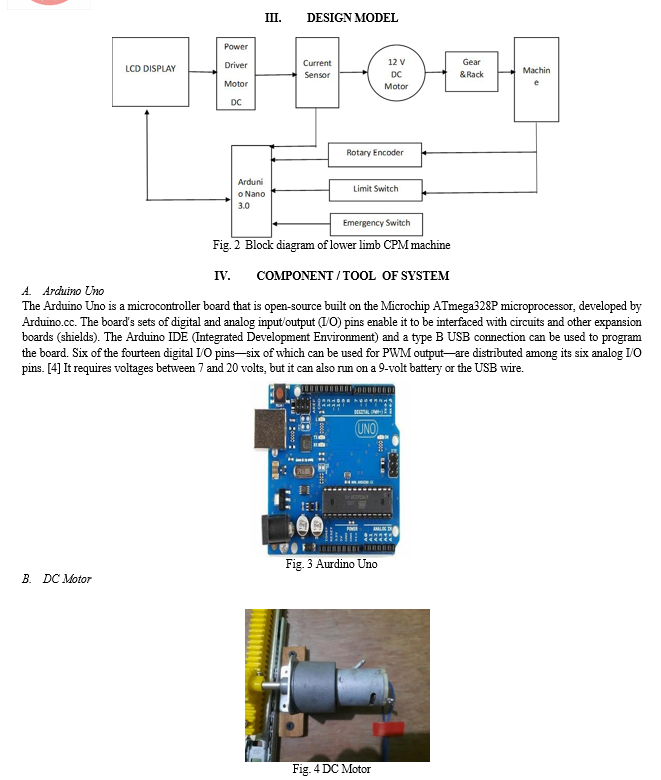
The model consists of a plywood foundation with a stainless steel main frame, bearing, and caster wheel for smooth movement. The sliding mechanism consists of two metal plates and balls, with the bottom portion attached to the plywood and the upper portion attached to the rack. The rack and pinion system turns rotational motion into linear motion, having a gear meshing with a flat bar with teeth. The motor turns the pinion, causing the rack to move linearly, transforming the motor's rotational action into linear motion.
The rack is coupled to the main frame using linkage, pulling it and pushing it back to its starting position. When the motor's rotation is reversed, the rack moves in the other direction, forcing the main frame back to its initial position. This combination results in a recurrent back and forth motion, resulting in abduction movement.
Power supply is given by a main switch, which transforms AC current into DC current, which is communicated to the Arduino and motor. The Arduino runs the motor based on programming circumstances such as motor direction, delay, and speed. When the rack extends to the extreme position, it strikes the limit switch, actuating the current circuit and opening the other circuit, creating the back and forth movement. A switch is attached to this circuit for on and off circuit connections.
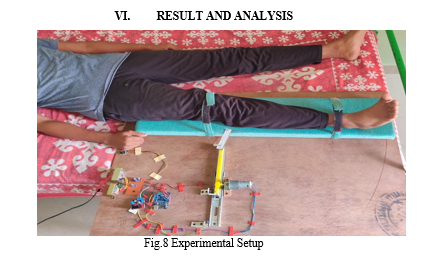
Table I Test Results
|
Tests |
Range of motion in Degree ° |
Time for complete movement in (s) |
Delay (s) |
|
1 |
35 |
16 |
0 |
|
2 |
35 |
18 |
2 |
|
3 |
35 |
19 |
3 |
|
4 |
35 |
20 |
4 |
We have performed the activity from weight range of 10 to 25 kg weight of the leg and machine works perfectly for hip joints movement. These are the outcome we have found after experimentation on the lower limb cpm machine. So Result after testing are found to be satisfactory.
The study aimed to determine the benefits of continuous passive motion (CPM) in physiotherapy for patients undergoing total hip arthroplasty (THA). Results showed that CPM significantly improved hip range-of-motion and facilitated regaining movement. Patients with CPM reported lower pain levels and less hospital stay, but did not increase analgesic requirements or wound drainage. The study recommends an optimum CPM regime for patients. CPM can help maintain normal periarticular soft tissue compliance and prevent stiffness by pumping blood and edema fluid away from the joint and periarticular tissues. However, long-term improvements are yet to be demonstrated, and evidence supporting routine use of CPM machines is lacking. To fully utilize CPM's clinical application, factors such as preoperative ROM, postoperative day of CPM initiation, daily ROM increment, and total application days must be considered.
Conclusion
In conclusion, the introduction of Continuous Passive Motion (CPM) machines into our rehabilitation project has proven to be crucial in aiding the recovery process following joint injury or surgery. By focusing on enhancing mobility, reducing stiffness, and preventing problems such as adhesions, CPM therapy has played a vital role in optimizing results for patients undergoing hip joint rehabilitation. Through joint efforts with healthcare specialists and attention to established guidelines, we have successfully integrated CPM therapy as a significant component of our rehabilitation approach. By utilizing motorized devices to repetitively move the afflicted joint within specified parameters, we have been able to commence therapy in the hospital setting and easily transition to home-based rehabilitation with the use of a home unit. Consultation with physiotherapists and strict adherence to prescribed treatment regimens have helped us to fulfill our project objectives effectively, while minimizing difficulties during therapy. The employment of CPM machines has not only simplified the restoration of joint function but has also contributed greatly to enhancing the overall quality of life for our patients. In essence, our investigation highlights the crucial importance of CPM therapy in post-injury or surgery joint rehabilitation, validating its place as a cornerstone intervention for maximizing patient outcomes and fostering long-term recovery.
References
[1] T. Deaconescu, A. Deaconescu, and I. Petre, \"Continuous passive motion-based rehabilitation equipment for the recovery of lower limb bearing joints,\" International Journal of Biomechatronics and Biomedical Robotics, vol. 3, no. 1, pp. 12, 2014. [2] C. J. Chevillotte, M. H. Ali, R. T. Trousdale, and M. W. Pagnano, \"Variability in Hip Range of Motion on Clinical Examination,\" The Journal of Arthroplasty, vol. 24, no. 5, pp. 693–697, Aug. 2009. [3] C. H. Guzmán, A. Blanco, J. A. Brizuela, and F. A. Gómez, \"Robust control of a hip–joint rehabilitation robot,\" Biomedical Signal Processing and Control, vol. 35, pp. 100–109, May 2017. [4] T. B. Palmer, N. D. Jenkins, and J. T. Cramer, \"Reliability of manual versus automated techniques for assessing passive stiffness of the posterior muscles of the hip and thigh,\" Journal of Sports Sciences, vol. 31, no. 8, pp. 867–877, Apr. 2013. [5] R. Vatovec, J. Maruši?, G. Markovi?, and N. Šarabon, \"Effects of Nordic hamstring exercise combined with glider exercise on hip flexion flexibility and hamstring passive stiffness,\" Journal of Sports Sciences, vol. 39, no. 20, pp. 2370–2377, Jun. 2021. [6] M. Vasanthakumar, B. Vinod, J. K. Mohanta, and S. Mohan, \"Design and Robust Motion Control of a Planar 1P-2P RP Hybrid Manipulator for Lower Limb Rehabilitation Applications,\" Journal of Intelligent & Robotic Systems, vol. 96, no. 1, pp. 17–30, Dec. 2018. [7] R. Trochimczuk, T. Ku?mierowski, and P. Anchimiuk, \"Study of CPM Device used for Rehabilitation and Effective Pain Management Following Knee Alloplasty,\" International Journal of Aplied Mechanics and Engineering, vol. 22, no. 1, pp. 241–251, Feb. 2017. [8] H. Husted, \"Fast-track hip and knee arthroplasty: clinical and organizational aspects,\" Acta Orthopaedica, vol. 83, no. sup346, pp. 1–39, Oct. 2012. [9] N. B. Foss, M. T. Kristensen, and H. Kehlet, \"Anaemia impedes functional mobility after hip fracture surgery,\" Age And Ageing, vol. 37, no. 2, pp. 173–178, Mar. 2008. [10] M. J. Philippon, M. Ryan, M. B. Martin, and J. Huard, \"Capsulolabral Adhesions After Hip Arthroscopy for the Treatment of Femoroacetabular Impingement: Strategies During Rehabilitation and Return to Sport to Reduce the Risk of Revision,\" Arthroscopy, Sports Medicine, and Rehabilitation, vol. 4, no. 1, pp. e255–e262, Jan. 2022. [11] J. S. Penny, O. Ovesen, J. Varmarken, and S. Overgaard, \"Similar range of motion and function after resurfacing large–head or standard total hip arthroplasty,\" Acta Orthopaedica, vol. 84, no. 3, pp. 246–253, Mar. 2013. [12] A. M. Chaudhari, S. T. Jamison, M. P. McNally, X. Pan, and L. C. Schmitt, \"Hip adductor activations during run-to-cut manoeuvres in compression shorts: implications for return to sport after groin injury,\" Journal of Sports Sciences, vol. 32, no. 14, pp. 1333–1340, Mar. 2014. [13] H. MS, \"Effectiveness of Continuous Passive Motion in Hemiarthroplasty of Hip,\" Journal of Medical Science and Clinical Research, vol. 6, no. 2, Feb. 2018. [14] A. Lenssen and R. de Bie, \"Role of physiotherapy in peri-operative management in total knee and hip surgery,\" Injury, vol. 37, pp. S41–S43, Dec. 2006. [15] J. Edelstein, A. Ranawat, K. R. Enseki, R. J. Yun, and P. Draovitch, \"Post-operative guidelines following hip arthroscopy,\" Current Reviews in Musculoskeletal Medicine, vol. 5, no. 1, pp. 15–23, Feb. 2012. [16] S. Mehta and J. Roy, \"Systematic review of home physiotherapy after hip fracture surgery,\" Journal of Rehabilitation Medicine, vol. 43, no. 6, pp. 477–480, Jun. 2011. [17] H. Tanino, T. Sato, Y. Nishida, R. Mitsutake, and H. Ito, \"Hip stability after total hip arthroplasty predicted by intraoperative stability test and range of motion: a cross-sectional study,\" BMC Musculoskeletal Disorders, vol. 19, no. 1, Oct. 2018. [18] K. E. Davis, M. A. Ritter, M. E. Berend, and J. B. Meding, \"The Importance of Range of Motion after Total Hip Arthroplasty,\" Clinical Orthopaedics & Related Research, vol. 465, pp. 180–184, Dec. 2007. [19] C. Guzmán-Valdivia, A. Blanco-Ortega, M. Oliver-Salazar, F. Gómez-Becerra, and J. Carrera- Escobedo, \"HipBot – The design, development and control of a therapeutic robot for hip rehabilitation,\" Mechatronics, vol. 30, pp. 55–64, Sep. 2015. [20] I. Dominik and R. Dwornicka, \"Selection of Drives for Prototype of Continuous Passive Motion Machine,\" Applied Mechanics and Materials, vol. 759, pp. 51–57, May 2015. [21] V. H. Palaniappan and S. S. Mohamed, \"Design of Automated Physiotherapy Device for Knee Rehabilitation Using TRIZ,\" Proceedings of the International Colloquium on Sports Science, Exercise, Engineering and Technology 2014 (ICoSSEET 2014), pp. 459–473, Dec. 2014. [22] 22] P. Linek, P. E. Muckelt, D. Sikora, N. Booysen, and M. Stokes, \"Assessing Movement Quality in Youth Footballers: The Relationship between Hip and Lower Limb Movement Screen and Functional Movement Screen,\" Applied Sciences, vol. 11, no. 19, Oct. 2021. [23] J. Cao, S. Q. Xie, R. Das, and G. L. Zhu, \"Control strategies for effective robot assisted gait rehabilitation: The state of art and future prospects,\" Medical Engineering & Physics, vol. 36, no. 12, pp. 1555–1566, Dec. 2014. [24] E. Akdo?an and M. A. Adli, \"The design and control of a therapeutic exercise robot for lower limb rehabilitation: Physiotherabot,\" Mechatronics, vol. 21, no. 3, pp. 509–522, Apr. 2011. [25] U. Demir, S. Kocao?lu, and E. Akdo?an, \"Human impedance parameter estimation using artificial neural network for modelling physiotherapist motion,\" Biocybernetics and Biomedical Engineering, vol. 36, no. 2, pp. 318–326, 2016. [26] D. Bradley, C. Acosta-Marquez, M. Hawley, S. Brownsell, P. Enderby, and S. Mawson, \"NeXOS – The design, development and evaluation of a rehabilitation system for the lower limbs,\" Mechatronics, vol. 19, no. 2, pp. 247–257, Mar. 2009. [27] J. Wu, J. Gao, R. Song, R. Li, Y. Li, and L. Jiang, \"The design and control of a 3DOF lower limb rehabilitation robot,\" Mechatronics, vol. 33, pp. 13–22, Feb. 2016.
Copyright
Copyright © 2024 Prof. Manish Dakhore, Navneet Shelke , Samyak Meshram, Yash Kuhikar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Download Paper
Paper Id : IJRASET62407
Publish Date : 2024-05-20
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here
 Submit Paper Online
Submit Paper Online