

Ijraset Journal For Research in Applied Science and Engineering Technology
Prolong Sitting: A Metabolic Health Risk among White-collar Workers: A Review Article
Authors: Nwokoleme Vincent , Modestus Nwogu C, Kizito Praise-God D, Salami Emmanuel O
DOI Link: https://doi.org/10.22214/ijraset.2023.55005
Certificate: View Certificate
Abstract
This article is about the metabolic health risks involved with prolonged sitting also known as sedentary lifestyle. Our bodies are designed to move, and research has shown that sedentary lifestyles increase health risks. In addition to type 2 diabetes, cancers, and cardiovascular diseases, sedentary lifestyles can lead to premature mortality. Often times a sedentary activity such as prolonged sitting is overlooked, when in fact, sitting for long periods of time has a negative effect on health. The goal of this presentation is to research and spread awareness about the health risks involved with prolonged sitting. In order to spread awareness, we have explored most of the common health risk associated with prolong sitting and as well made some crucial recommendations that are needed to elicit the right attitude to prolong sitting among individuals. This topic address sedentary lifestyles as a problem and display what a sedentary lifestyle looks like. It went further to discuss the problem of prolonged sitting and potential solutions. Although there are resources that already exist on the topic of sedentary lifestyles. We have created resources specific to the individuals in order to be more effective in spreading awareness to them. This is a widespread problem with serious consequences, yet simple fixes. This is an attempt to spread awareness to a population that includes individuals at a critical point in life who may not be informed about this issue. Methodology: Two electronic data-bases (Green Science Hub, and Free full PDF) were searched for empirical and non-empirical studies that measured/ talked about at least one key outcome focusing on sedentary lifestyle.The non-empirical study was lifted from page 1 to 10 of each of the data-bases search results, producing a total of 67 review articles.Search terms included: Sedentary lifestyle, metabolic disorder, prolong sitting, and white collar workers.The searched terms were further limited to TITLE/ABSTRACT/KEYWORDS. The search was also limited to “non-empirical studies” and “empirical studies”, in “Health”, Published in “the last ten (10) years” (January, 2013 to July, 2023), and published in ‘English’. Study Selection: Inclusion Criteria The inclusion criteria for this systematic review were full-length research articles contained in peer-reviewed academic journals in English language. Only empirical and non-empirical studies published January, 2013 up to May, 2023 were qualified. Also research included only the population of white-collar workers. Research that presented one metabolic outcome was selected. Study Selection: Exclusion Criteria Contents from materials such as Abstracts, Conference presentations, Presentations on posters, Letters to editors, books or book chapters, proposals for dissertations/Thesis, validation studies, proposal protocols and retrospective design were excluded.A total of 67 research related articles were searched in the electronic data-bases, 37 from Green Science Hub and 30 articles fromFree full PDF, of which 15 were excluded on the basis that they were not full articles, leaving a total of 52 articles. 25 articles were further screened out on the basis report included bed-ridden population in addition to sedentary lifestyle. 7 articles were further screened out as they were conference papers. Therefore, 12 studies from Green Science Hub and 8 studies from Freefull PDF were reviewed in total.
Introduction
I. INTRODUCTION
Our bodies are made to move and that is why physical activity is important. It is unrealistic to eliminate physical inactivity completely, but inactivity becomes a concern when it turns into sedentary behaviour. Prolong sitting includes sitting for long time during commuting, while working, in the home, and as a part of leisure time (Owen, Healy, Matthews, & Dunstan, 2010). In physiological terms, sedentary behaviour is defined to be any behaviour during waking hours that requires an energy expenditure of less than 1.5 METs, which are multiples of the basal metabolic rate (Ainsworth, Haskell, Whitt, Irwin, Swartz &Strathet al, 2000). To put this into perspective, brisk walking expends energy worth 3-4 METs and running expends energy worth 8-9 METs (Ainsworth et al., 2000).
Therefore, activities such as watching television or working at a desk can be determined to be sedentary behaviour due to the low energy expenditure involved in those activities. Prolonged sitting is the main source of sedentary behavior that people encounter and fortunately it is a behaviour that can be modified.
The findings of some studies indicated that for each two-hour increment in sitting time, the risk of obesity and diabetes increases by 5% and 7%, respectively. In contrast, prolonged sitting behavior raises the risk of musculoskeletal disorders, especially low back pain. Additionally, the findings of Gianoudis (2008) revealed that a greater overall sitting time is associated with an increased risk of sarcopenia, which climbs by 33% for each one-hour increment of sitting.
Other studies have shown that sedentary occupations are associated with a higher risk of developing some types of cancers, such as colorectal, ovarian, prostate, and endometrial cancer (Engeroff, Fuzeiki, Vogt &Banzer, 2017). Another outcome of a sedentary lifestyle is premature death.
The World Health Organization (WHO, 2013) estimates that 3.2 million people worldwide die prematurely each year due to a sedentary lifestyle. Studies have shown that people who spend almost all of their working time in a sitting position have a 1.4-times greater chance of premature death after 12 years than their counterparts who sit for less time at work.
A. Understanding Prolong Sitting
Prolong sitting in this presentation has been explained in terms of sedentary behaviour. Sedentary behaviour has been defined as “any behavour r characterized by an energy expenditure of ≤1.5 METs while in a sitting or reclining posture’’ (Cart, 2012). The results of Church et al.’s (2011) study revealed that the average energy expenditure of individuals while at work declined from 1960-2010. This shift in occupational energy expenditure has been associated with a decrease of 100 calories per day, which in turn account for as much as 80% of the average increase in body weight among the working population during this same period.
B. Population Mostly Exposed to Prolong Sitting
Modern workplaces have shifted the nature of occupations from active to sedentary and promote lengthy sitting behavour. One cause of this change is the transition from paper-based work to computerized and paperless work (Church, Thomas, Tudor-Locke, Katzmarzyk, Earnest,Rodarte, Martin, Blair & Bouchard, 2011).
Office workers are part of a large group of occupations that generally work in a sitting position for much of the day (Office for National Statistics of UK, 2012).
These people remain in a sitting posture for about two-thirds of their working hours, and their bouts of sitting periods typically last at least 30 minutes (Evan, 2012). An Australian study revealed that 42% of men and 47% of women spend an average of 6.3 of their 8-hour shifts in sedentary and sitting jobs (Chau, 2012)
C. Why is Prolonged Sitting so Common?
Simply put, prolonged sitting is ubiquitous. Since the middle of the last century, physical, economic and social environments have been quickly changing (Owen, Sugiyama, Eakin, Gardiner, Tremblay, Sallis, 2010).
These changes in society have led to lifestyles that involve significant reductions in the demands for physical activity and therefore, energy expenditure (Thorp, Owen, Neuhaus & Dunstan, 2011).
In homes, workplaces, schools, modes of transportation, and recreational venues, there are always opportunities and in many cases, requirements to sit (Dunstan, Howard, Healy, & Owen, 2012).
Furthermore, jobs have evolved to involve more and more sitting time. In 1970, two in ten working Americans had jobs that required only light activity (predominantly desk job), where as in 2000, more than four in ten working Americans were in light activity jobs (Owen, Sparling, Healy, Dunstan, & Matthews, 2010). Developments such as televisions, computers, cell phones, and video games have also created unlimited opportunities for people of all ages to sit for long periods of time. Over the past 20 years, total screen time has increased dramatically, as computers, phones, and televisions have become a part of everyday life for people of all ages (Owen, et a., 2010).
Prolonged sitting involves a unique set of behaviours and unique consequences that are independent of those involved in the absence of moderate to vigorous physical activity (Owen, et al, 2010). Therefore, awareness of sitting time, awareness of the health risks involved with prolonged sitting, and the lack of understanding on the differences between too much sitting and too little exercise act as significant contributions to the problem.
D. Effect of Prolong Sitting on Health
According to the US National Health and Nutrition Examination Survey (2003-2004, 2005-2006), the majority of adults surveyed spent waking time in sedentary behaviour (58%) or light-intensity activity (39%) and only 3% in exercise time. The popularity of sedentary behavior is concerning because sedentary lifestyles are associated with an increased risk for more than 35 chronic diseases/conditions and increased mortality rates (Thyfault, Du, Kraus, Levine, & Booth, 2015). The body is made to move, and thus, not moving will pose negative effects throughout all the systems of the body. Data collected from many studies show that inactivity and low levels of activity are associated with increased risk for cardiovascular diseases, obesity, type 2 diabetes, cancer, and increased mortality risk (Engeroff, Fuzeki, Vogt, &Banzer, 2016).
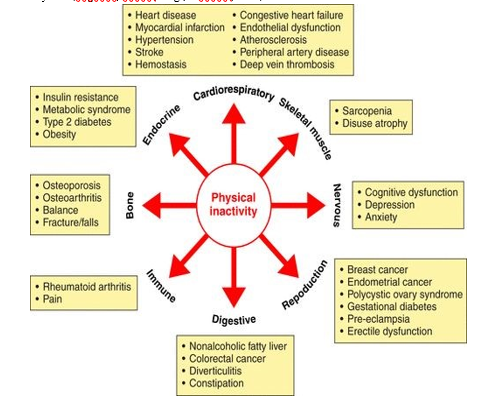
This diagram displays the different body systems that physical inactivity can have an effect on and the specific conditions or diseases within each body system that are associated with physical inactivity (Booth, Roberts, Thyfault, Ruegsegger & Toedebusch, 2017)
E. Relationship between Sedentary Lifestyles and Sitting
The term sedentary was derived from the Latin term “sedere” which means “to sit”
(?Dabundo, Sidman, &Fiala, 2015). While sedentary behaviours can describe a variety? of activities for different purposes and in different contexts, time spent sitting is the overall representation of what sedentary behaviour primarily involves (Dabundoet al, 2015). In other words, sitting time is the main contributor to sedentary behaviours.
Attempting to make changes to one’s lifestyle can be intimidating. However, an easier way to look at it is to think about the amount of time spent sitting each day. While sedentary behaviors are “different activities, for different purposes in different contexts”, sitting time is a “generic descriptor covering what these sedentary behaviours primarily involve” (Owen et al, 2010). The many periods of sitting that we engage in each day is what actually makes up our sedentary lifestyles and it seems a little less intimidating to think about adjusting the time we spend sitting as opposed to our lifestyles.
F. Effect of Prolonged Sitting on Metabolic Health
Prolonged sitting is associated with many health risks such as obesity, type 2 diabetes, vitamin deficiencies, hypercholesterolemia, muscle/skin changes, cardiovascular conditions, and cancer (?Boothet al, 2017). Obesity is a worldwide healthproblem that affects over 100 million people (Inyang& Stella, 2015). Spending long periods of time sitting leads to the accumulation of excess calories which is essentially weight gain, and eventually obesity if the individual’s caloric intake is greater than their calories expended (Inyang& Stella, 2015). The total cost in America of the effects of obesity, including income lost from decreased productivity and hospitalization, and premature mortality were approximately 147 billion dollars in 2008 (WHO, 2018). ?Some? of the other conditions associated with obesity include hypertension, diabetes, cancer, and osteoarthritis (Inyang& Stella, 2015).
Type 2 diabetes, also known as non-insulin dependent diabetes, is a result of the body’s inability to utilize insulin effectively (Inyang& Stella, 2015). Prolonged sitting behaviors are strongly associated with increased eating, weight gain, and increased screen time, all of which are major risk factors for type 2 diabetes (Brannon &Feist,?2007). Research has shown that nine out of ten cases of type 2 diabetes could have? been prevented if risk factors of weight, diet, smoking, and inactivity were addressed (Inyang& Stella, 2015). However, research has also shown that the absence of exercise is not what lead individuals to diabetes, but rather, the amount of time spent sitting that can increase the risk (Inyang& Stella, 2015). Research has shown that prolong sitting behaviour has a direct effect on vascular health, metabolism, and bone mineral content, all of which contribute to chronic diseases (Tremblay, Colley, Saunders, Healy, & Owen, 2010). While physical inactivity has long been viewed as a minor risk factor for chronic diseases, a systematic review of 14 literature on the relationship between physical activity and prevention of coronary heart disease (CHD) has shown that physical inactivity is in fact a strong independent risk factor for CHD (Powell, Thompson, Caspersen& Kendrick, 1987). According to the American Heart Association (AHA, 1992), physical activity improved glucose tolerance, increased fibrinolysis (breaking of clots), and reducing blood pressure; all of which play a role in metabolic health. Of equal importance, long periods of sitting can cause a reduction in bone mineral density which can lead to negative health outcomes (Tremblay et al, 2010). While environmental and genetic factors contribute to an individual’s risk for CHD, behavioral factors such as physical inactivity are aspects of life that individuals have control over. The American Heart Association (1992) Researchers calculated risk of coronary heart disease (CHD) due to inactivity to be a greater risk than those who have high cholesterol and those who smoke cigarettes (AHA, 1992). However, it is similar to the risk ratio for hypertension (high blood pressure), which is related to metabolic health risks. Sedentary individuals have about twice the chance of experiencing CHD than physically active individual (Powers &Howley, 2012).
CHD is associated with atherosclerosis, which is a gradual narrowing of arteries serving the heart due to thickening of the inner lining of the artery by fatty plaque (Powers & Howley, 2012). Physical inactivity is one of the behavioural risk factors that interact with other risk factors to cause atherosclerosis (Powers & Howley, 2012). Atherosclerosis is the leading contributor to heart attack and stroke deaths (AHA, 1992). It is the narrowing of the artery that will result in reduction of blood flow to the heart therefore leading to a heart attack (Powers & Howley, 2012). It has been thought that the danger of atherosclerosis is occlusion, however, most heart attacks and strokes result from rupture of the plaque which then block blood flow, a process referred to as “inflammation” (Libby, Okamoto, Rocha, & Folco, 2010). Inflammation is linked to several chronic diseases such as hypertension, coronary heart disease, stroke, cancers, respiratory conditions, type 2 diabetes and the metabolic syndrome (Mathur & Pedersen, 2008). Inflammation is described to be a significant increase in inflammatory cytokines (Powers & Howley, 2012). When there is too much adipose tissue present in the body, there are more hormones and inflammatory cytokines released by the adipose tissue (Gustafson, 2010).
Increased inflammatory cytokines circulate and interfere with insulin, which is described to be insulin resistance (Gustafson, 2010). Insulin resistance is a reduced ability to take up glucose at a given insulin concentration and is linked to type 2 diabetes and metabolic syndrome in addition to CHD (Powers & Howley, 2012). Furthermore, increased levels of physical activity are associated with decreased levels of inflammation (Powers & Howley, 2012). As muscles are used in physical activity, they produce the same types of inflammatory cytokines that lead to inflammation and it can be significantly increased as a result of physical activity (Brandt & Pedersen, 2010). This physical activity induced reduction of inflammation however, involves a different process than that which causes inflammation (Brandt & Pedersen, 2010). The cytokinase, IL-6 can act both as an inflammatory and anti-inflammatory depending on the circumstances (Brandt & Pedersen, 2010). Therefore, as a result of physical activity, IL-6 works to inhibit the effect of some inflammatory cytokines and increases the concentration of anti-inflammatory cytokines (Powers & Howley, 2012). Thus, physical activity helps to reduce inflammation that can lead to chronic diseases including coronary heart disease.
Some aspects of vascular health relate directly to metabolic health and how it is affected by physical inactivity. It was mentioned that hypertension has a strong risk ratio with inactivity, similar to the risk for CHD (Powers & Howley, 2012). Hypertension is extremely common, affecting more than 68 million Americans (Gillespie, Kuklina, Briss, & Hong, 2011). It has been found that hypertension tends to occur alongside of metabolic abnormalities - obesity, insulin resistance, and dyslipidemia (elevated triglyceride levels) (Powers & Howley, 2012).
The coexistence of the conditions are referred to as metabolic syndrome or the deadly quartet if obesity is present (Powers & Howley, 2012). Insulin is a hormone that aids with the uptake of glucose, in other words, the body’s ability to use glucose (Powers & Howley, 2012). Because insulin resistance reduces the ability for the body to utilize glucose, blood glucose concentrations increase when insulin resistance occurs. When there are increased blood glucose concentrations, the pancreas secretes more insulin in the attempt to maintain homeostasis (Powers & Howley, 2012). However, if the pancreas cannot keep up with the increasing demand for insulin, the blood glucose concentration remains higher than normal, which is the characteristic of type 2 diabetes (Powers & Howley, 2012). Furthermore, individuals with insulin resistance tend to have greater free fatty acid (FFA) levels which can lead to increased plasma triglycerides (Powers & Howley, 2012).
Elevated triglyceride/FFA levels are associated with low levels of lipoprotein lipase (LPL) because LPL is a rate limiting enzyme that regulates the uptake of circulating free fatty acids into adipose tissue and skeletal muscle (Hamburg, 2007). Research has shown that acute and chronic sedentary behaviour causes a reduction in LPL activity (Hamburg, 2007). There is a strong inverse relationship between LPL activity and risk for coronary heart disease (Hamilton, Hamilton, &Zderic, 2004). Therefore, decreased levels of LPL activity are linked to increased risk for cardiovascular disease, increased circulating triglyceride levels, and decreased high-density lipoprotein cholesterol (HDL) cholesterol - all of which may contribute to risks that have been frequently observed to occur during metabolic diseases such as obesity, type 2 diabetes, and coronary heart disease (Hamilton, 2004). It has been found that even fragmentary reductions in LPL activity were associated with increased risk for mortality and coronary heart disease (Hamilton, 2004).
G. What are the Effects on the Skeletal System?
Similar to most body parts, the muscular and skeletal system are ever-changing and constantly adapting to the needs of the body. If you don’t use it, you lose it. The body will not work and put energy towards a part of the body that does not need it. It is inevitable for the body to slowly deteriorate over time, especially with age, however, inactivity, accelerates this deterioration. People who sit more than five hours a day are at risk for losing 1% of muscle strength per day (Inyang& Stella, 2015). In addition to the reduction in capacity and strength of the muscle, the communication between the muscle cells and the brain cells also decrease as they are not used as much (Inyang & Stella, 2015). It is specifically the bone mineral density that is decreasing over time with inactivity. (Caillot-Augusseau, 1998). Zerwekh and colleagues (1998) found that in healthy individuals 1-4% of bone mineral density was lost from bone in lumbar spine, femoral neck, and greater trochanter after a period of inactivity. One theory as to why this loss of bone mineral density occurs is that inactivity affects the processes and rates of bone breakdown and buildup, however, other studies (Kim, 2003). (Zwart, 2007) have found that bone formation is for the most part unaffected by inactivity. Sedentary behaviour will still lead to a greater rate of bone reabsorption than formation which is how bone mineral density is lost after prolonged inactivity. However, even though inactivity has a slow deterioration effect on bone health, exercise did not have the ability to prevent reduction in bone mineral density (Tremblay et al, 2010).
H. Sitting and Intermittent Breaks
Not only is it important to consider the amount of time spent sitting, but also how the prolonged time of sitting is accumulated. In other words, does the sitting occur in one full bout with no interruption? Or are there breaks throughout the periods of sitting. The single bouts of prolonged inactivity decrease insulin sensitivity in healthy humans and have been proven to affect lipid metabolism as well
II. RECOMMENDATIONS
- Office workers and individuals on high risk of prolong sitting should adopt lifestyle changes that will permit intermediate exercise even at work.
- Manufacturing industries should help design office furniture and equipment that can improve ergonomics to help mitigate prolong sitting operation.
- More publications should be made to help create awareness on the health risks of prolong sitting
Conclusion
The health risks involved with prolonged sitting is an important issue to spread awareness about, especially as it continues to become more prevalent in society. Excessive sitting significantly increases risk for chronic diseases, but these risks can also be reduced by simply taking breaks throughout long durations of sitting. Sitting with intermittent breaks or sitting with incorporated sitting is the best and most simple solution to the problem of too much sitting. Another important finding to keep in mind is that the benefits of exercise do not counteract the detrimental effects of prolonged sitting. Furthermore, college students exhibit poor physical activity maintenance, therefore indicating the necessity of spreading awareness throughout campus. There were a few students who took a flyer from the display and a handful of students who were intrigued by the poster and discussing it. Methods of spreading awareness to college students were not completely ineffective, but could be improved to have a greater impact. Potential changes for future projects may include a change in medium and/or change in display sites.
References
[1] Ainsworth, B. E., Haskell, W. L., Whitt, M. C., Irwin, M. L., Swartz, A. M., Strath, S. J., . . . Leon, A. S. (2000). Compendium of Physical Activities: An update of activity codes and MET intensities. Medicine & Science in Sports & Exercise, 32(9 Supplement): S498-504. doi:10.1097/00005768-200009001-00009 [2] Bey, L. & Hamilton, M. T. (2003). Suppression of skeletal muscle lipoprotein lipase activity during physical inactivity: a molecular reason to maintain daily low-intensity activity. The Journal of Physiology, 551: 673-682. doi:10.1113/jphysiol.2003.045591 [3] Bhatt, A. (2018, April 09). Cholesterol: Understanding HDL vs. LDL. Retrieved from https://www.health.harvard.edu/blog/understanding-cholesterol-hdl-vs-ldl-2018041213608 [4] Booth, F. W., Roberts, C. K., Thyfault, J. P., Ruegsegger, G. N., Toedebusch, R. G. (2017). Role of inactivity in chronic diseases: evolutionary insight and pathophysiological mechanisms. Physiological reviews, 97(4), 1351-1402. [5] Brannon, L &Feist, J. (2007). Health Psychology An Introduction to Behaviour and Health 6th Edition, United State of America, Thomspon Wadsworth Publisher. [6] Buckworth, J. & Claudio, N. 2004. Physical activity, exercise, and sedentary behaviorin college students. Journal of American College Health, 53 (1), 28-34. [7] Bullock, V. E., Griffiths, P., Sherar, L. B., &Clemes, S. A. (2017). Sitting time and obesity in 46 a sample of adults from Europe and the USA. Annals Of Human Biology, 44(3), 230-doi:10.1080/03014460.2016.1232749 [8] Buman, M. P., Kline, C. E., Youngstedt, S. D., Phillips, B., de Mello, M. T., &Hirshkowitz, M. (2015). Sitting and Television Viewing. Chest, 147(3), 728-734. doi:10.1378/chest.14-1187 [9] Butler, K. M., Ramos, J. S., Buchanan, C. A., &Dalleck, L. C. (2018). Can reducing sitting time in the university setting improve the cardiometabolic health of college students? Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, Volume 11, 603-610. doi:10.2147/dmso.s179590 [10] Carlson, S. A., Fulton, J. E., Pratt, M., Yang, Z., & Adams, E. K. (2015). Inadequate Physical Activity and Health Care Expenditures in the United States. Progress in Cardiovascular Diseases, 57(4), 315-323. doi:10.1016/j.pcad.2014.08.002 [11] Clee, S. M., Zhang, H., Bissada, N., Miao, L., Ehrenborg, E., Benlian, P., Shen, G. X., Angel, A., LeBoeuf, R. C., & Hayden, M. R. (1997). Relationship between lipoprotein lipase and high density lipoprotein cholesterol in mice: modulation by cholesteryl ester transfer protein and dietary status. The Journal of Lipid Research, 38, 2079-2089. [12] Dabundo, M. L., Sidman, C. L., &Fiala, K. A. (2015). Sitting Behavior and Physical Activity of College Students. International Journal of Adult Vocational Education and Technology, 6(3), 61-doi:10.4018/ijavet.2015070105 [13] Dunstan, D. W., Howard, B., Healy, G. N., & Owen, N. (2012). Too much sitting – A health 47 hazard. Diabetes Research and Clinical Practice, 97(3), 368-376. doi:10.1016/j.diabres.2012.05.020 [14] Edwards, M. K., &Loprinzi, P. D. (2018). High Amounts of Sitting, Low Cardiorespiratory Fitness, and Low Physical Activity Levels: 3 Key Ingredients in the Recipe for Influencing Metabolic Syndrome Prevalence. American Journal Of Health Promotion, 32(3), 587-594. doi:10.1177/0890117116684889 [15] Engeroff, T., Fuzeki, E., Vogt, L., Banzer, W. (2016). Breaking up sedentary time, physical activity and lipoprotein metabolism. Goethe-University Frankfurt, Department of Sport Medicine, 20(2017), 678-683. doi.org/10.1016/j.jsams.2016.11.018 [16] *Ekelund, U., Steene-Johannessen, J., Brown, W. J., Fagerland, M. W., Owen, N., Powell, K. E., Bauman, A., Lee, I. (2016). Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. The Lancet, 388(10051), 1302-1310. doi:10.1016/S0140-6736(16)30370-1 [17] Flint, S. W., Crank, H., Tew, G., & Till, S. (2017). \"It\'s not an Obvious Issue, Is It?\" Office-Based Employees\' Perceptions of Prolonged Sitting at Work: A Qualitative Study. Journal Of Occupational & Environmental Medicine, 59(12), 1161-116 doi:10.1097/JOM.0000000000001130 [18] Fountaine, C. J., Johann, J., Skalko, C., &Liguori, G. A. (2016). Metabolic and energy cost of sitting, standing, and a novel sitting/stepping protocol in recreationally active college students. International Journal of Exercise Science, 9(2), 223-229. [19] Gilson, N. D., Burton, N. W., Van Uffelen, J. G., Brown, W. J. 2011. Occupational sitting 48 time: employee’s perceptions of health risks and intervention strategies. Health Promotion Journal Australia, 22(1), 38-43. [20] Gillespie, C., Kuklina, E. V., Briss, P. A., Blair, N.A., & Hong, Y. Vital signs: prevalence, treatment, and control of hypertension - United States, 1999-2002 and 2005-2008. Morbidity and Mortality Weekly Report, 60, 103-108. [21] Gummelt, A. (2015, June 3). Physical Activity vs. Exercise: What\'s the Difference? Retrieved from https://www.acefitness.org/education-and-resources/lifestyle/blog/5460/physic al-activity-vs-exercise-what-s-the-difference [22] Gustafon, B. (2010). Adipose tissue, inflammation and atherosclerosis. Journal of Atherosclerosis and Thrombosis, 17, 332-341. [23] Hamburg, N. M., McMackin, C. J., Huang, A. L., Shenouda, S. M., Widlansky, M. E., Schulz, E., Gokce, N., Ruderman, N. B., Keaney, J. F., … Vita, J. A. (2007). Physical inactivity rapidly induces insulin resistance and microvascular dysfunction in healthy volunteers. Arteriosclerosis, thrombosis, and vascular biology, 27(12), 2650-6. doi: 10.1161/ATVBAHA.107.153288 6 [24] Hamilton, M. T., Hamilton, D. G., &Zderic, T. W. (2004). Exercise physiology versus inactivity physiology: an essential concept for understanding lipoprotein lipase regulation. Exercise and sport sciences reviews, 32(4), 161-6. [25] Inyang, M. P., & Stella, O., (2015). Sedentary Lifestyle: Health Implications. IOSR Journal of Nursing and Health Science, 4(2), 20-25. doi: 10.9790/1959-04212025 [26] Katzmarzyk, P. T., Church, T. S., Craig, C. L., & Bouchard, C. (2009). Sitting Time and Mortality from All Causes, Cardiovascular Disease, and Cancer. Medicine & Science in Sports & Exercise, 41(5), 998-1005. doi:10.1249/mss.0b013e3181930355 [27] Kim, H., Iwasaki, K., Miyake, T., Shiozawa, T., Nozaki, S. &Yajima, K. (2003). Changes in bone turnover markers during 14 day 6 degree head-down bed rest. J. Bone Miner. Metab. 21(5), 311-315. [28] Lewis, B., Napolitano, M., Buman, M., Williams, D., &Nigg, C. (2017). Future directions in physical activity intervention research: expanding our focus to sedentary behaviors, technology, and dissemination. Journal Of BehavioralMedicine,40(1), 112-126. doi:10.1007/s10865-016-9797-8 [29] Libby, P., Okamoto, Y., Rocha, V. Z., &Folco, E. (2010). Inflammation in atherosclerosis. Circulation Journal 74, 213-220. [30] Lynch, B. M., & Owen, N. (2015). Too Much Sitting and Chronic Disease Risk: Steps to Move the Science Forward. Annals Of Internal Medicine , 162 (2), 146-147. doi:10.7326/M14-2552 [31] Manson, J. E., Skerrett, P. J., Greenland, P., Vanitallie, T. B. (2004). The escalating pandemics of obesity and sedentary lifestyle. A call to action for clinicians. Archives of Internal Medicine, 164(2), 249-58. [32] Mathur, N., & Pedersen, B. K. (2008). Exercise as a Mean to Control Low-Grade Systemic Inflammation. Mediators of Inflammation, 2008, 1-6. doi:10.1155/2008/109502 [33] Messing, K., Stock, S., Côté, J., &Tissot, F. (2015). Is Sitting Worse Than Static Standing? How a Gender Analysis Can Move Us Toward Understanding Determinants and Effects of Occupational Standing and Walking. Journal Of Occupational & Environmental Hygiene, 12(3), D11-D17. doi:10.1080/15459624.2014.987388 [34] Moulin, M. S., Irwin, J. D. (2017). An assessment of sedentary time among undergraduate students at a Canadian university. International Journal of Exercise Science 10(8), 1116-1129. [35] Ngomo, S., Messing, K., Perrault, H., Comtois, A. (2008). Orthostatic symptoms, blood pressure and working postures of factory and service workers over an observed workday. Appl. Ergon. 39,729736. [36] Owen, N., Bauman, A., & Brown, W. (2008). Too much sitting: A novel and important predictor of chronic disease risk? British Journal of Sports Medicine 43(2), 81-83. doi:10.1136/bjsm.2008.055269 [37] Owen, N., Healy, G. N., Matthews, C. E., & Dunstan, D. W. (2010). Too Much Sitting: The Population-Health Science of Sedentary Behavior. Exercise and Sport Sciences Reviews, 38(3), 105–113. http://doi.org/10.1097/JES.0b013e3181e373a2 [38] Owen, N., Sparling, P. B., Healy, G. N., Dunstan, D. W., & Matthews, C. E. (2010). Sedentary Behavior: Emerging Evidence for a New Health Risk. Mayo Clinic Proceedings, 85(12), 1138-1141. doi:10.4065/mcp.2010.0444 [39] Pate, R. R., O’Neill, J. R., Lobelo, F. (2008). The evolving definition of “sedentary”. Exercise and Sport Sciences Reviews, 36(4), 173-178. doi: 10.1097/JES.0b013e3181877d1a [40] Powell, K. E., Thompson, P. D., Caspersen, C. J., & Kendrick, J. S. (1987). Physical activity 51 and the incidence of coronary heart disease. Annu rev public health, 8, 253-287. [41] Powers, S. K., &Howley, E. T. (2012). Exercise physiology: Theory and application to fitness and performance. New York: McGraw-Hill Higher Education. [42] Thorp, A. A., Owen, N., Neuhaus, M., & Dunstan, D. W. (2011, August). Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996-2011. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/21767729 [43] Thyfault, J. P., Du, M., Kraus, W. E., Levine, J. A., & Booth, F. W. (2015). Physiology of sedentarybehavior and its relationship to health outcomes. Medicine and science in sports and exercise, 47(6), 1301-5. doi: 10.1249/MSS.0000000000000518 [44] Tremblay, M. S., Colley, R. C., Saunders, T. J., Healy, G. N., Owen, N. (2010). Physiological and health implications of a sedentary lifestyle. Application physiological nutrition metabolism, 35(6), 725-40. doi: 10.1139/H10-079 [45] Van der Ploeg, H. P., Chey, T., Korda, R. J., Banks, E., Bauman, A. (2012). Sitting time and all-cause mortality risk in 222497 Australian adults. Arch Intern Medicine, 172 (6), 494-500. [46] Wang, H., &Eckel, R. H. (2009). Lipoprotein lipase: from gene to obesity. Am J PhysiolEndocrinolMetab., 297(2), 271-288. doi: 10.1152/ajpendo.90920.2008 [47] Wendel, M. L., Benden, M. E. (2017). Standing vs sitting time in stand-biased classrooms. AJPH Letters and Responses, 107(3). [48] WHO (2008). Urbanization and Health. Bulletin of the World Health Organization.
Copyright
Copyright © 2023 Nwokoleme Vincent , Modestus Nwogu C, Kizito Praise-God D, Salami Emmanuel O. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Download Paper
Paper Id : IJRASET55005
Publish Date : 2023-07-25
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here
 Submit Paper Online
Submit Paper Online